Prenatal screening for genetic conditions has become a complex process with a multitude of tests to choose from. With advancing technology, the available options are becoming overwhelming for both health care professionals and patients. It can be difficult to understand all of the options and decide what is best for you. Below is a review the common prenatal screening options that are available along with the pertinent limitations and benefits of each.
It is important to remember that all of the following are OPTIONAL during a pregnancy. Prenatal screening for chromosome abnormalities should be made available to all women during all pregnancies (as recommended by the American Congress of Obstetricians and Gynecologists). Certainly there are women who choose not to have any prenatal screening done. Many women like to have the information provided by these tests to prepare for when the baby is born. Other women may use the information to guide decisions such as termination and adoption. In discussing these testing options I am not advocating for or protesting against the issue of abortion. My goal is to take a nondirective approach of explaining the commonly available prenatal screening options.
Topics Discussed
- What are Chromosome Abnormalities?
- Age Related Risk
- First Trimester Screening (the nuchal translucency test)
- Second Trimester Screening (the quad screen)
- Other Screening Options
- Noninvasive Prenatal Testing (Materniti21, Verifi, Panorama, Harmony)
- Diagnostic Testing
What Are Chromosome Abnormalities?
To understand what a chromosome abnormality is we have to take a step back and talk about some basic genetics.
Typically, we have 23 pairs of chromosomes in each cell of our body. A chromosome is made up of tightly wound DNA and can be thought of as a genetic blue print that determines everything from our hair color to our risk for genetic disease. The first 22 pairs of chromosomes are called autosomes and the last pair are the sex chromosome (XX for girls and XY for boys). For each chromosome pair, we inherit one chromosome from our mother and one chromosome from our father. During meiosis, a process of cell division, sex cells (sperm and eggs) are created that contain only one copy of each chromosome. This is important so that when the sperm fertilizes the egg there are a total of 46 chromosomes (half from mom and half from dad). However, sometimes errors are made in this process that can cause some of the sperm cells and egg cells to have extra or  missing chromosomes. This is called nondisjunction. For example, if one of the sex cells has an extra chromosome 21, the resulting fetus will have three copies of chromosome 21 instead of two. This is called trisomy 21 (see image), but is more commonly referred to as Down syndrome. Down syndrome is a common chromosome abnormality, occurring in approximately 1 in every 800 recognized pregnancies. A trisomy can occur in any chromosome pair, but most will result in an early miscarriage before you even know you’re pregnant. Two other chromosomal trisomies that are sometimes compatible with life and those are trisomy 18 and trisomy 13. Both of these chromosome abnormalities are more severe than Down syndrome and are generally considered fatal conditions. Most pregnancies with trisomy 13 or 18 will result in a miscarriage. If the pregnancy makes it to term, the vast majority of babies won’t live past 1 year of life.
missing chromosomes. This is called nondisjunction. For example, if one of the sex cells has an extra chromosome 21, the resulting fetus will have three copies of chromosome 21 instead of two. This is called trisomy 21 (see image), but is more commonly referred to as Down syndrome. Down syndrome is a common chromosome abnormality, occurring in approximately 1 in every 800 recognized pregnancies. A trisomy can occur in any chromosome pair, but most will result in an early miscarriage before you even know you’re pregnant. Two other chromosomal trisomies that are sometimes compatible with life and those are trisomy 18 and trisomy 13. Both of these chromosome abnormalities are more severe than Down syndrome and are generally considered fatal conditions. Most pregnancies with trisomy 13 or 18 will result in a miscarriage. If the pregnancy makes it to term, the vast majority of babies won’t live past 1 year of life.
For a more detailed discussion of chromosomes and chromosome abnormalities check out this link.
Before any prenatal testing is performed, a risk approximation for chromosome abnormalities can be given based on maternal age. As a woman get older, the risk for chromosome abnormalities in a pregnancy increases. Below is an example of a maternal age risk chart. It provides a specific risk for Down syndrome and a risk for all chromosomes abnormalities (which includes Down syndrome, trisomy 18, and trisomy 13). A mother’s risk decreases as the pregnancy progresses due to the risk of natural miscarriage.

Risk for “All” chromosome abnormalities include Down syndrome, Trisomy 18, and Trisomy 13


First off, it’s important to know that a “screening” test will just provide you with a more accurate risk assessment. It cannot be used to diagnose or rule out a chromosome abnormality in a pregnancy. This is a first tier test that can either be reassuring or help guide decisions about potential follow-up testing.
The first part of the test involves an ultrasound that will measure the nuchal translucency (NT). The NT is an accumulation of fluid at the base of the baby’s neck that is expected to be seen in all pregnancies. A measurement above 3.0-3.5mm is considered to be “abnormal.” An increased NT is associated with a higher risk for chromosome abnormality or structural defect (like a heart defect).
The second part of the 1st trimester screen involves a blood draw from the mother that will measure two proteins that are made by the pregnancy (PAPP-A and hCG).
A risk assessment for the pregnancy will be calculated based on the NT measurement, protein levels from the blood draw, and numerous other factors (maternal age, ethinicity, diabetics, ect.). The detection rate for Down syndrome is 83% with a false positive rate of 5%. The detection rate for trisomy 18 is approximately 80% with a false positive rate of <1%.
The 1st trimester screen is available between 11-14 weeks gestational age. Depending on the laboratory/hospital, results are usually reported within one week. Results will be reported as a risk assessment for both Down syndrome and trisomy 18. The result could come back as high as a 1 in 2 chance (50% chance the baby has Down syndrome). Alternatively, the risk could be extremely low (ex. 1 in 10,000 chance the baby has Down syndrome). Of course the numbers could fall anywhere between the two extremes. Regardless of the result, it important to remember that this test cannot diagnose or rule out either chromosome abnormality, it’s just providing you with more information.
The test will also be reported as “positive” or “negative.” For example, anyone with a Down syndrome risk greater than a 1 in 270 chance will be considered “positive.” The cut-off between a positive and negative test will vary between labs. Of course, a positive result does not mean the baby has a chromosome abnormality. It simply means that the risk in increased. Here’s an example:
A woman does a first trimester screen and her risk for Down syndrome is 1 in 100 and her risk for trisomy 18 is 1 in 10,000. This would be a negative test for trisomy 18 but a positive test for Down syndrome. A 1 in 100 risk is equivalent to a 1% risk. In other words there is a 99% chance the pregnancy does not have Down syndrome, but because there is an increased risk (above the 1:270 cut-off) this individual will likely be offered additional testing options. (see diagnostics tests and/or non-invasive prenatal testing)
Second Trimester Screening (The Quad Screen)
The obvious difference between the quad screen and the 1st trimester screen is the timing. Another key difference is that along with screening for Down syndrome and trisomy 18 it will also screen for neural tube defects (like spina bifida).
The quad screen is just a blood draw. This test will be looking at four proteins that are made by the pregnancy (AFP, hCG, UE3, DIA). The protein levels will be measured and used to calculate the risk assessment (factors such as maternal age, ethnicity, ect. are again contributory).
The detection rate for Down syndrome is approximately 80% with a false positive rate of 4-5%. The detection rate for trisomy 18 is 80% with a false positive rate of <0.5%. Lastly, the AFP protein is used to screen for open neural tube defects with a detection rate of 80%.
There are multiple other screening options that incorporate combinations/variations of the 1st trimester screen and the quad screen. For detailed sensitivity and specificity of the tests see the table below.
- Full Integrated Screen: This test combines the first trimester screen and the quad screen to increase the overall detection rate for chromosome abnormalities. The main downside is that you won’t receive results until both the first and second trimester test are performed and analyzed.
- Serum Integrated Screen: This test is the same as the full integrated screen except there is no ultrasound as part of the 1st trimester screen (it’s just two separate blood draws). Results will also not be available until both tests are completed. This may be an ideal option for women whose insurance does not cover an ultrasound (or have a limited number of ultrasounds in a pregnancy).
- Sequential Screen: This test is almost the exact same as the full integrated screen. The only difference is that you will receive preliminary results after the first trimester screen. The overall detection rate for Down syndrome is just slightly lower when compared to the full integrated screen.
- Triple Screen: Same test as the quad screen except it analyzes three proteins instead of four (therefore the detection rate is slightly decreased).
- AFP only (second trimester): Having AFP protein measured during the second trimester is a way to screen for open neural tube defects (ONTD). Of course, the AFP protein is already part of integrated screen, sequential screen, and quad screen. Therefore, this test would only be made available to women who only had a 1st trimester screen but would also like to screen for ONTD in the second trimester (80% detection rate). A second trimester targeted ultrasound is another way to screen for ONTD, with an even higher detection rate (see below).
- Second Trimester Targeted Ultrasound: A targeted ultrasound during the second trimester (ideally between 18-20 weeks) is another way to screen for chromosome abnormalities, birth defects, and other signs of genetic disease. The majority of babies that have a chromosome abnormality will also have an abnormal ultrasound finding (possibly multiple findings). Therefore a normal second trimester ultrasound certainly decreases the risk that your baby has a chromosome abnormality or other birth defect. The detection rate for ONTD is approximately 95% (99% for the more severe cases).

Afp4: aka Quad Screen
FPR: False Positive Rate
OAPR: Odds of being Affected giving a Positive Result
(This table is from Integrated Genetics, a LabCorp Specialty Testing Group)
All of the above mentioned tests are prenatal screening tests that should be made available to all women in all pregnancies. In the following sections I will discuss noninvasive prenatal testing and diagnostic testing through CVS or amniocentesis. These tests will not necessarily be discussed or offered to all women. They are generally recommended to be offered to women who are at an increased risk for a chromosome abnormality. Factors that put women in the increased risk category may include advanced maternal age ≥35, ultrasound anomalies, a positive screening test, or a previous pregnancy with chromosome abnormality.
Benefits:
- Screens for Down syndrome, trisomy 18, trisomy 13, and sex chromosome abnormalities at a high detection rate
- May screen for smaller chromosome changes such as microdeletions
- There is not risk to the baby, it’s just a blood draw from the mother
- It can be done as early as week 10 in a pregnancy
Limitations
- Still considered a screening test, although it is highly accurate it is still possible to have a false positive or false negative
- Insurance coverage is sometimes tricky
Noninvasive prenatal testing (NIPT) is a newer technology that is able to isolate fragments placental DNA from a sample of the mothers blood (using cell-free fetal DNA technology). The test is able to screen for Down syndrome, trisomy 18, trisomy 13, and sex chromosome abnormalities with a high detection rate. There are no risks to the mother or the baby because it just involves a blood draw from the mother. The testing can be done as early as week 10 in a pregnancy and results are typically reported within 1-2 weeks.
Even though studies have shown that this testing has high detection rates a low false positive rate, it’s still considered a screening test (not diagnostic). If a person has a positive test it is still recommended to confirm the result through a diagnostic procedure (CVS or amniocentesis). Conversely, a negative test would significantly reduce the likelihood of the pregnancy having a chromosome abnormality but it cannot rule it out. One explanation for a false positive test is whats called confined placental mosaicism (CPM). As I mentioned above, NIPT is testing placental DNA and does not directly test the baby’s DNA. In about 1-3% of pregnancies, the genetics of the placenta can be different from the genetics of the baby. This can lead to false positives (or false negatives).
These tests are often advertised to patients and healthcare providers as >99% accurate. It is important to recognize this is a population-level statistic and only applies to the entire population of women screened. It does not apply to an individual’s result. Since most pregnancies are unaffected and most results are “low risk” or “negative” this test is correct 99% of the time for all women. However, the probability a high risk result indicates an affected fetus is not 99% in the majority of cases. In order to determine how likely a high risk result indicates an affected fetus, you need to know the positive predictive value (PPV). The PPV reflects the chance that a positive test result is a true positive. If you have a positive result, it is important to have a discussion with a genetic counselor or health care provider who is familiar with the PPV of this testing. One helpful resource that can be used is an online NIPT PPV calculator.
Insurance coverage for this test is complicated. As of now most insurances will cover testing for women with certain risk factors. These risk factors may include advanced maternal age ≥35, ultrasound anomalies, a positive screening test, and a previous pregnancy with chromosome abnormality. If insurance is not covering the test and you are paying out of pocket, the cost could be upwards of $1000-$2000 dollars. Some labs will have a policy to limit your out-of-pocket cost.
There are numerous companies that are offering this testing. Each lab is a little different in terms of their detection rates, cost, and how they report results. Here is a list of the labs and the name of their test:
(click on the links to see specific detection rates and other information)
Sequenom: Materniti21 Plus Prenatal Test
Progenity (previously Verinata): Verifi Prenatal Test
Natera: Panorama Prenatal Test
Ariosa Diagnostics: Harmony Prenatal Test
*Important Definitions:
Sensitivity: The number (or percentage) of positive test results that are actually positive. (Ex. A positive test for Down syndrome and the baby actually has Down syndrome)
Specificity: The number (or percentage) of negative test results that are actually negative. (Ex. A negative test for Down syndrome and the baby does not have Down syndrome)
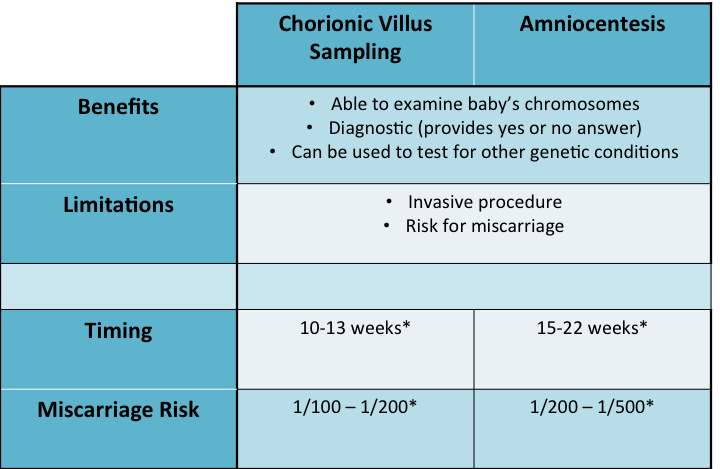
*Timing and miscarriage risk may vary depending on the hospital or physician
Chorionic villus sampling (CVS) and amniocentesis are the gold standard for prenatal diagnosis. Both usually involve inserting a needle guided by ultrasound through the abdomen of the mother to sample either the chorionic villus (CVS) or amniotic fluid (amniocentesis). These samples contain fetal cells which are then sent to a laboratory. The lab is able to use the sample to get a picture baby’s chromosomes, this is called a karyotype. Next they count the chromosomes to see if there any are extra or missing. This is considered a diagnostic test because in looking at the baby’s chromosomes the lab is able to confirm or rule out a diagnosis of a chromosome abnormality (Down syndrome, trisomy 18, trisomy 13, or any other).
Preliminary results from either test can be reported as early as 24-48 hours after sending in the sample. These preliminary results are done using a technique called fluorescence in situ hybridization (FISH) and just look at certain chromosomes (21, 18, 13, and the sex chromosomes). The FISH analysis is highly accurate (>99%). The final chromosome analysis, in which the full picture of the chromosomes is analyzed, usually takes 1-2 weeks. Most of the time, the final chromosome analysis just confirms what we already knew from the FISH results.
Both the CVS and amniocentesis are considered an invasive test and have an associated risk for miscarriage. The risk for CVS is about 1 in 100 to 200, while the risk for amniocentesis is about 1 in 200 to 400. While this is a low risk it is certainly important to be aware of this before having either test done. The miscarriage risk may vary depending on the hospital or physician.
Another key difference between the CVS and amniocentesis is the timing. The CVS is a first trimester test available between 11-13 weeks gestation while the amniocentesis is a second trimester test that is usually done between 15-22 weeks gestation.
There are also other genetic tests that can be performed from a CVS or amniocentesis sample. One such test is called a microarray. A microarray essentially takes a detailed scan of the chromosomes and looks for any missing or extra pieces that are too small to be visualized on a conventional chromosome analysis. Small pieces of missing or extra chromosome material can sometimes be associated with birth defects, mental retardation, and other medical concerns. However, if a genetic change is found on a microarray analysis it can sometimes be difficult to predict its significance. Some of these genetic changes are benign while others have a more severe impact. An example of a situation in which a microarray might be ordered is for a woman who has multiple ultrasound anomalies. The woman has an amniocentesis to look for a chromosome abnormality and the chromosome studies are normal. She and her doctor decide to order a microarray to look for smaller chromosome changes that could potentially explain the ultrasound findings. Most of the time the test can be done from the amnio sample that was already collected.
Lastly, either a CVS or amniocentesis can be used to test for known genetic conditions in the family. For example, a couple had a previous child with cystic fibrosis and they want to if their current pregnancy also has cystic fibrosis. The couple had genetic testing done after their first pregnancy to find that they were both carriers for a genetic mutation in the cystic fibrosis gene. Therefore, there is a 25% risk to future pregnancies to also have cystic fibrosis. A specific genetic test for cystic fibrosis can be performed on a sample from a CVS or amniocentesis to see if the current pregnancy is affected.

{kind=link}
Please feel free to leave your comments, questions, or any additional topics you would like discussed.
Thanks for putting together that very nice overview. I am a 46 year old surgeon so a very “elderly primagravida” and this was not a planned pregnancy. A lot has changed since I was in med school (only really recall CVS and amnio being available). Had a dating u/s a few weeks ago and now off to the NT screen and meeting with genetic counselor in 2 days. Know I am at high risk for aneuploidy and even as a medical professional, wasn’t quite sure of the difference between the Harmony and quad screen testing that I am sure will be next up on the plate. Found this page thru BabyCenter. Thanks
I am so glad I found your site. I have very little medical training. I’m a career FF/EMT, so outside of being a “road doctor”, I am self taught. I recently had a stillbirth, my son Jake, at 24wks. They think he passed around 21.5wks, based off of his measurements. I had prenatal screening and I honeslty do not remember the numbers that spit out at me but I do remember being told they weren’t too high but one was on a little on the end. I do remember his NT scan was 2.9. There was a cyst on his brain, left temporal area, that they said would probably go away on its own, then the fetal cardiologist was concerned with a possibly coarctation of his aorta. When we went for the follow up with the fetal cariologist is when my Jake no longer had a heartbeat. I delivered him the next day. 10inches and 10ounces of love. We had bloodwork, tissue sample and an autopsy. The tests came back showing he had a partial duplication of chromosome 1. I have been searching for info and its so hard to find anything…there is so much about 12,18 and 21. Please, can you tell me where to look or share any knowledge you may have on this. I am 34yrs old and we want to try again. Its scary to think of potentially feeling so much loss and pain for another child if this should happen again. Please help.
First off, I’m sorry for your loss but thanks for sharing your story. Do you remeber if the duplication was identified on the chromosome karyotype or did they also perform a microarray? These smaller chromosome changes can be difficult to interpret sometimes. A partial deletion or duplication can happen on any chromosome and can vary greatly in size. Whenever one of these changes is identified, the next step is to see what genes are involved in the duplicated area and if other patients have been reported with the same or similar finding. For whatever reason, some deletions/duplications happen more frequently than others and we have a better understanding of them. Other times it will be the first reported of its kind and is difficult to interpret its significance. To help with the interpretation of the particular duplication identified in your pregnancy I would have to have more information about size and location (which should be on the report). Another step is to perform chromosome studies on yourself and your partner to see if this duplication was inherited. That helps us to understand its significance and also if there would be an increased risk for future pregnancies. A lot of labs will perform these parental studies free of charge. Most of the time they are not inherited and are just “de novo” or new changes happening for the first time when the sperm meets the egg. There was certainly nothing either you or your partner did to cause this.
Thank you for the very informative post. I’m struggling with the decision of amniocentesis vs. Panorama. I’m 39 and my NT Scan (1.3) with blood work came back at 1 in 1,262 risk for DS. A lot of mothers-to-be seem to be struggling with invasive/diagnostic vs. non-invasive/risk assessment. Any suggestions?
It’s certainly a personal choice. I would say most of my patients are starting with non-invasive testing and going from there. If it’s negative they likely feel reassured enough, and if it’s positive they can still consider an amnio to confirm the diagnosis.
For yourself, you’ve already had some reassurance with the normal screening test. A 1,262 risk for Down syndrome is essentially the equivalent risk of a 20-year old woman in the first trimester. It comes down to how you view the invasive procedure. Some women do not want to have an increased risk for miscarriage no matter what the circumstance (even though the risk is small). Other women want the most reliable information possible.
I am definitely doing the Harmony or Maternit21 test and the NT ultrasound, but I am unsure if I should also do the Sequential prenatal blood screening tests. Do you recommend doing all of these tests? My concern is the quad test results may give me extra stress since it is not as accurate the cell free DNA test and will give me Also, do you prefer the Maternit21 or Harmony test? Thank you for any guidance!
I don’t have a particular preference between the labs that offer NIPT. The technologies are all quite similar. Between MaterniT21 and Harmony, they do report results differently. MaterniT21 will actually say positive or negative for each chromosome abnormality, while Harmony will say high risk or low risk (<1 in 10,000). It is still considered a screening test so giving a number versus +/- is probably more appropriate. Regardless, it's essentially the same.
I do have patients who elect to do NIPT and also a serum screening test (1st screen w/ NT, quad screen, or sequential). In terms of screening for chromosome abnormalities, NIPT is going to screen for more things and at a higher detection rate. Therefore one could argue that a serum screening test is unnecessary. A second trimester serum screen will screen for neural tube defects as an added benefit. Although a targeted ultrasound to look at the brain and spinal cord has a higher detection rate. Also if there is a particular protein serum level that is extremely high or extremely low, that can have other implications other than chromosome abnormalities. Overall I would say there are minor benefits to having serum screening done in conjunction with NIPT, but it's a reasonable option.
I am going in for a CVS, but want to know what it screens for……every chromosomal abnormality or only the most common? Do I have to tell the doctor which things I want to screen for?
Thank you so much for your reply. I just reread your site and it is so helpful. It’s hard to find information comparing all the information. I am 14 weeks pregnant now and due n December. I originally planned on doing one of the NIPT tests but am now leaning towards skipping it but I don’t want to have any regrets. So far I have done the first trimester blood test and the NT ultrasound. I will be doing the 2nd trimester blood draw next week. My only risk factor is that I will be turning 36 next month. Here are my results:
CRL= 60.4 mm 12 Weeks 4 Days EDC=December 14, 2014
Nuccal Translucency = 1.42 mm
Age Risk Downs= 1 in 296
NT Screening Down’s Risk = 1 in 2900
Trisomy 18 Risk = 1 in 73000
PAPP-A = 1.21 MOM
bHCG= 1.47 MOM
Delta NT= 0.91 MOM
I feel confident with these results but wondering if I should still go ahead with the NIPT. I have a high deductible and would likely have to pay $800 for the harmony test plus $150 to see the genetic counselor. I know it’s a personal decision but am wondering how you guide your patients when their tests come back with a low risk. Would you still recommend NIPT testing since it is more accurate? Thank you for your much appreciated help.
Your numbers look reassuring thus far. It certainly is a personal decision and I try not to steer people one way or the other, but since you asked I’ll give you my opinion. I would wait for now and see how things look on the targeted ultrasound (usually done around 18-20 weeks). Most babies with a chromosome abnormality will have an identifiable abnormality. If everything looks good on ultrasound, your risk for down syndrome would be closer to 1 in 6000. If there are any ultrasound abnormalities, then perhaps you could consider additional testing (amnio or NIPT).
Thanks for your opinion. I really appreciate it.
Do you have any information on the reliability of the new MaterniT21 Plus with “Enhanced Sequencing Series?” We just got a result from that of a 1p36 deletion, but the lab said they have only ever had that result with one other person and cannot say the likelihood of a false positive.
There are a number of the NIPT labs that are now testing for chromosome deletions such as 1p36 and others. I’m not exactly sure how MaterniT21 is reporting those, but early studies are suggesting a high accuracy (>99%). However, it is just a screening test so it’s possible to have a false positive. A level II targeted ultrasound to look for any abnormalities could be helpful (although not all babies with 1p36 deletions will have identifiable abnormalities).
Well, it turns out my result was wrong. Amnio with some kind of in-depth sequencing (sorry I forgot the name but it took a week) showed that my baby is fine. Sequenom told my genetic counselor that of the three babies who tested positive for 1p36, two were false positives (one of them was me.) For cri-du-chat, two of four were false positives. They don’t have any more data than that – which makes me think that they have released this new part of the test prematurely. My ultrasound is next week, but based on the amnio, we don’t expect anything to look wrong.
First off- I just want to say — wow. What a special and thoughtful person you are to take the time to respond to so many parents to-be who are probably as confused as I am about what’s what in all the testing. It’s a true act of kindness and I hope that your heart is full knowing how appreciated your input is by so many. I’m 38 and turn 39 in June, two days after the due date of my baby. I’m 15 weeks and 6 days. I took the MaterniT21 and my results all came back normal/good for that. I had the nuchal and while the neck measurements were really good, my blood work was not good and showed a high risk. I’m still confused if that’s affected by my age? I’m thinking to go ahead and do amnio but is that necessary? Thank you for your guidance. I sincerely am appreciative.
It would probably be most helpful just to have a discussion with your primary provider or genetic counselor (if available). It’s difficult to know why the blood work on the first trimester screen showed a high risk. It’s most likely just a normal variation. I would feel very reassured at this point with the normal MaterniT21. I would say your next step could be a level II ultrasound at around 20 weeks to access the fetal anatomy. If everything is normal that will provide even more reassurance and if there were any concerns an amniocentesis could still be considered at that time.
I had a free cell dna test, I am 38 YO and did not do a sequential creen since I didnt find out I was pregnant until after the timeframe (pregnant on pill). My results are as follows. Apprently there may be some abnormalities, but my first ultrasound at 16 weeks and second at twenty both show normal growth and development and although it was too late for a sequential creen there were no signs of any abnormaites on the ultrasound. I don’t want an Amnio as this carries risk of misccariage. Do most abnormalites show on ultrasound? Could this be minor abnormality or none at all or is it more commonly somethign serious… Have ahd aweful anxiety since receiving these results…I will be seeing genetics couselor next week, but it seems they will simply suggest invasive procedures like Amnio…
– While this patient sample did not screen positive for trisomy
– of chromosome 13, 18, 21 the results were not consistent
– with the normal pattern expected. This result may be
– suggestive of abnormalities of other chromosomes not tested
– in this assay. Genetic counseling is recommended. For
– definitive diagnostic testing, follow-up options include CVS
– or amniocentesis. In addition, recent clinical evidence
– suggests that maternal malignancies may be detected using non
– invasive prenatal screening and should be included in the
– differential diagnosis.
It is difficult to say at this point. It’s important to keep in mind that any cell free fetal DNA test is a screening test and is not diagnostic. It’s reassuring that the ultrasound have been normal, but an ultrasound is not definitive either. From the report that you provided, they don’t actually mention what abnormalities were identified so it’s difficult for me to provide much insight.
The genetic counselor will certainly be able to provide more information regarding your particular result. An amnio will likely be offered but it is always optional. While there is a risk for miscarriage, it is likely very small. The risk associated with an amnio is often overstated and portrayed to be higher.
Thank you so much for this very helpful blog post. I am curious to know if you might have some advice for me, as I am facing the decision of whether or not to have an amnio. I am 38 years old and currently 13 weeks along. My cell-free DNA test (Panorama) came back with low-risk results across the board (<1/10,000.) My NT at 12 weeks/2 days was 1.5 and CRL was 5.86cm. However, my first trimester screening risk factor for Trisomy 21 was assessed as 1 in 54. I am told that this is due entirely to my age. (The Panorama results put my pre-test risk at 1 in 108, and that supposedly takes into account my age, so I am unsure of what is causing that discrepancy.) I am being offered an amnio at 16 weeks for 100% assurance. I am told the risk for a miscarriage due to amnio is about 1:1000. I also have a uterine anomaly (deeply bifurcated bicornuate uterus with unequal horns) because of which it took me several years to conceive. My right side uterus is too small to carry but the left side appears viable. I had one prior miscarriage, cause unknown. If there was no risk associated with the amnio, I would do the test because I would like to know definitively. A good result will put my mind at ease and a bad result will mean that I consider the very tough decision of whether to continue. But it has taken a lot of time and heartache to get this far along in what appears to be a healthy pregnancy — so I am very torn about taking a risk with an amnio. I would really appreciate your advice. Thank you in advance.
Depending on the reference they use, different labs will have different statistics for the pre-test risk that is quoted. Overall it sounds like the risk for trisomy 21 at this point is low. But an amnio always remains an option as the only diagnostic test in a pregnancy. It always comes down to weighing the potential risks against how you are feeling. Peace of mind is important especially if you think you’ll be anxious for the remainder of the pregnancy.
You could also wait and see how things look on a level II ultrasound at 18-20 weeks. If the fetal anatomy is completely normal you’ll get more reassurance that the risk is low. If there any any markers for Down syndrome identified you could still proceed with an amnio at that time.
We have unfortunately just received our harmony results which show an abnormality and is a high risk of trisomy 13.
Has anyone ever been told this and it been wrong? My wife is having the amnio this Thursday but we are already bracing ourselves for termination. It’s a horrible horrible time
Hello,
Sorry to hear this..we too had got the results as high risk for Edwards in our daughter.. we didn’t do amnio for the risk of miscarriage..as the risk for amnio was higher than the risk of Edwards.. I’m now 37 weeks pregnant and hope that all is well with my baby.. On the ultrasounds they could not find any markers for Edwards so they just told that we can avoid Amnio as my age may be causing higher risk to show.. we left it at that.. All the best.You wife would know what best to do.